
With so many articles in the archives and over a decade of writing to refer to, it’s fascinating to look back at how the contributors to this blog have examined emerging medical issues. Over the same period of this blog’s life, the availability of marijuana for medical use has expanded dramatically, paving the way for eventual legalization. Even very early on, this blog was cautious about the hype about its medical potential. The earliest post I can find was from 2009, when Peter Lipson wrote about its emerging use. He noted:
As marijuana becomes increasingly available for medical use, practitioners of science-based medicine need to evaluate the evidence for the use of this drug. In evaluating a new drug, we must ask a number of questions, including those of safety, efficacy, and perhaps redundancy. Claims for the efficacy of marijuana tend to be hyperbolic, with no condition being exempt from its benefits.
In 2014, David Gorski wrote a series of posts on medical marijuana, likening it to “the new herbalism” and noting:
It’s not enough just to say cannabis (or whatever cannabinoid drug or derivative you might wish to use) is “efficacious” against this disease or this condition. We need to know how efficacious it is compared to the existing standard of care.
The public enthusiasm for the recreational and medical use of marijuana is clear. Use has grown dramatically despite limited evidence. Now we have a study that helps to further clarify its potential role as a medicine. In a new paper published in the Journal of Clinical Oncology, researchers studied if cannabidiol (CBD) improved symptom control in patients with advanced cancer.
Cannabidiol (CBD) oil is one of the many chemical compounds called cannabinoids that are isolated from cannabis. Cannabis contains over 400 chemicals including at least 120 cannabinoids, which stimulate cannabinoid receptors in the body. (Yes, we have cannabinoid receptors and we even produce our own cannabinoids.) The most well-studied cannabinoids in the research setting are delta-9-tetrahydrocannabinol (THC) and CBD. CBD does not have the psychoactive profile of THC, and while it has been the source of considerable medical interest, its primary established role as a medical product is for the treatment of forms of childhood epilepsy.
Cannabidiol is a plausible and even promising treatment for the symptoms of advanced cancer. Patients with advanced stages of cancer can experience fatigue, anorexia and other distressing symptoms. Cannabis has been promoted as a more “natural” treatment option, so this study was designed to evaluate if CBD oil, in combination with standard pallative care, reduced patient symptom burden.
The trial
The study, titled “Phase IIb Randomized, Placebo-Controlled, Dose-Escalating, Double-Blind Study of Cannabidiol Oil for the Relief of Symptoms in Advanced Cancer (MedCan1-CBD)”, was a randomized, placebo-controlled study of CBD that took place in five medical centres in Queensland, Australia. Participants had advanced (palliative) cancer, and were over the age of 18 with symptoms causing distress (as measured by a standardized scoring tool), had no THC in their urine, and had adequate mobility (performance status) and cognitive function.
All patients in the study were to receive standard palliative care treatment. Patients were randomized to receive CBD oil (100mg/mL) or a matched placebo. Doses were increased gradually every third day, as they could tolerate, over 14 days, starting at 50mg once daily up to a maximum of 200mg three times daily. Patients were given the option of staying on the desired dose for two additional weeks.
Patients were assessed by telephone using a standardized instrument (assessing pain, fatigue, nausea, sleepiness, shortness of breath, appetite, anxiety, depression and overall well-being) every 3-4 days, with face-to-face assessments at days 14 and 28. This score, at day 14 compared to day zero, was the primary outcome measure. Secondary measures included individual symptom scores, pain control (as measured by oral morphine equivalents), and adverse events.
Results
Of 215 patients invited to participate, ultimately 144 participants were randomly assigned over a 33-month period. Two patients were eventually removed leading to 58 participants on CBD and 63 on the comparable placebo. The groups were comparable in terms of how many patients remained in the study at day 14 and day 28. Patient characteristics were comparable with the exception of the placebo group having a worse baseline symptom score at randomization.
Total symptom burden: Symptoms improved in both groups with no significant differences between the two group. (Symptoms actually improved more in the placebo group, but not significantly). Adjusted for the difference in the baseline score, there was basically zero difference between the two groups at day 14. There was also no difference in the proportion of “responders”, defined as a decrease in the symptom scale of six or more:
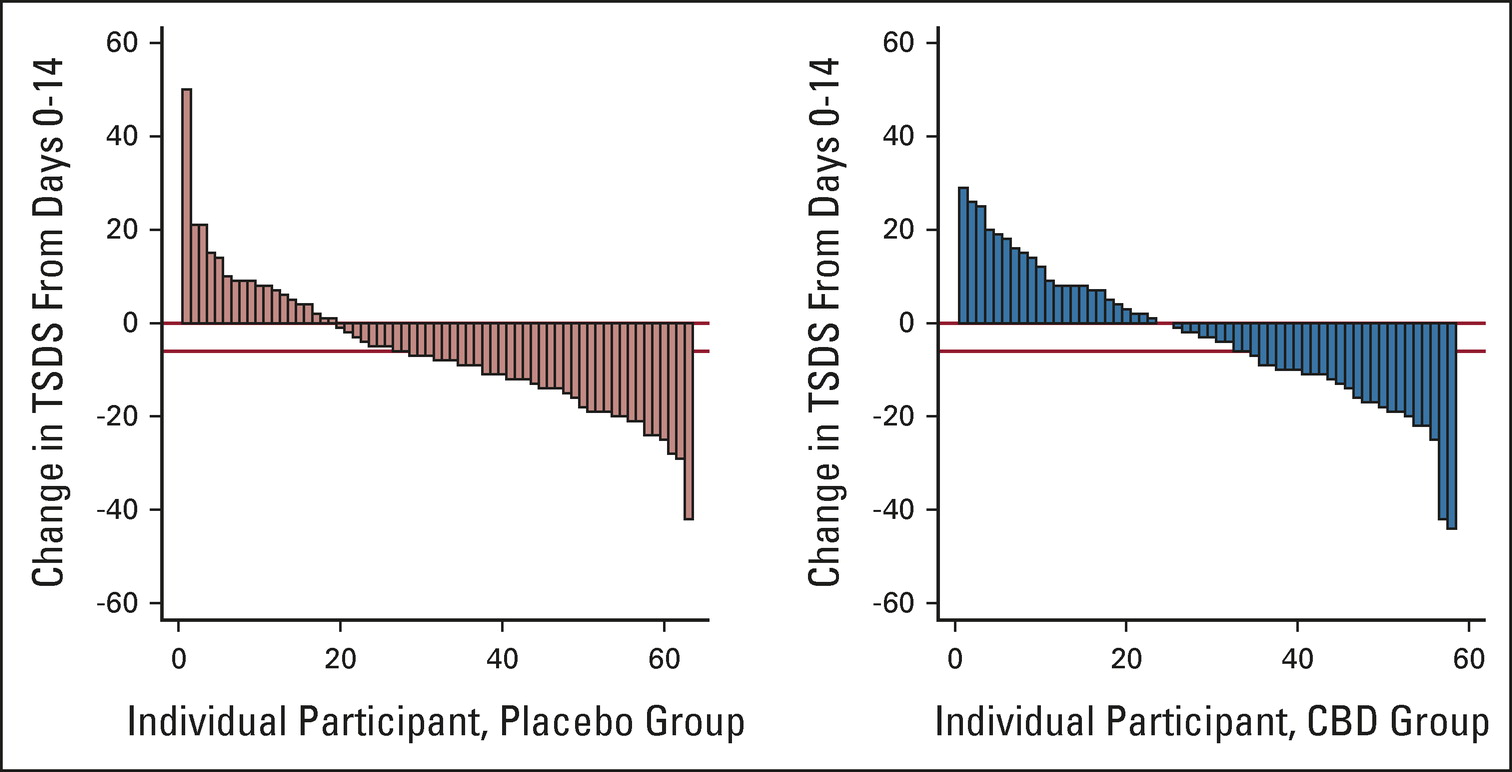
Proportion of responders (fall in Total Symptom Distress Score (TSDS) ≥ 6 between baseline and day 14) in each arm (placebo: 37 of 63 [58.7%]; CBD: 26 of 58 [44.8%], P = .13)
Change in individual symptoms: All measures in the symptom scale improved (fell) over time in both groups. There was no difference between groups in terms of physical, emotional, or well-being, or in any individual component (e.g., pain, nausea, appetite):
Participant-selected dose: The median final dose selected by participants was 6mL/day in the placebo group and 4mL/day in the CBD group (equivalent to a dose of 400mg/day).
Pain control: There was no difference detected between arms in terms of oral morphine equivalents used, or the changes in use over the duration of the study.
Other medications: There was no correlation between the participant-selected dose of CBD/placebo and opioid dose, or the use of drugs like benziodiazepines and antipsychotics.
Global impressions of change: Most participants reported feeling better or much better at day 14 and 28, often despite no change in the symptom score. There were no differences between the groups.
Adverse effects: There were no differences in events of special interest between the groups at days 14 and 28 in terms of adverse events, with a nonsignificant increase in somnolence and abdominal pain and a trend of more vomiting in the placebo group. In terms of other adverse events, there was a significant increase in shortness of breath reported in the CBD group. There were no differences in hospitalizations (none related to the study drug) or in overall survival.
Conclusion
While there has been significant enthusiasm in the use of cannabis as a medical treatment, this randomized controlled trial of CBD oil in patients found no benefit over standard care. Despite a plausible mechanism of action, CBD did not improve anxiety, depression, or any individual symptom substantially. CBD oil was well tolerated and there were few side effects with the possible higher rate of somnolence related to CBD use.
This trial differs from other research in that it was well-designed to minimize bias, used a standardized, verified CBD product, and was powered to detect if CBD offered any meaningful benefits. It measured effects using a validated scale that captures meaningful patient symptoms. The authors conclude:
This study has significant implications for policymakers regarding both approved indications for MC and its safe use. Medical cannabis has been approved in several countries for palliative care in the belief that it might improve the [quality of life] of patients with advanced disease. CBD is a popular cannabis product in the community as it has no psychoactive effects and does not impair driving ability. With current evidence, it is difficult to justify government subsidization of the cost of CBD nor recommend that patients pay for CBD products.
While no single study is definitive, this trial suggests that CBD, despite its popularity, may not offer any benefit to patients managing the symptoms of advanced cancer in a palliative setting.